
Introduction
In the past episode we spoke about anaesthesia in general, & we said that anaesthesia is a great discovery in medical studies since it help the surgical painful procedures to go on smoothly & without pain. At the same time we said that anaesthetic agents doesn’t follow a specific chemical category, neither they follow any specific mechanism of action, since there is a wide variety of agents which are used & different mechanisms combined at the same time to produce the pharmacological effects
In the past episode we spoke about anaesthesia in general, & we said that anaesthesia is a great discovery in medical studies since it help the surgical painful procedures to go on smoothly & without pain. At the same time we said that anaesthetic agents doesn’t follow a specific chemical category, neither they follow any specific mechanism of action, since there is a wide variety of agents which are used & different mechanisms combined at the same time to produce the pharmacological effects
In this part we’ll go more deeper discussing anaesthetic agents & their effects on the Nervous System in a more deeper & scientific manners
THE EFFECTS OF ANAESTHETICS ON THE NERVOUS SYSTEM
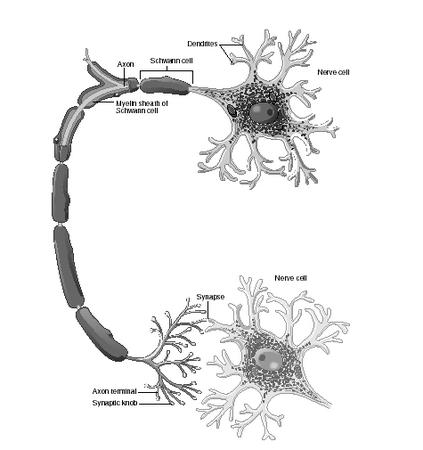
At the beginning & before discussing this topic, it is important to remember from the last lecture that there are 2 basic theories of anaesthetics actions which are the protein theory & the lipid theory, Now, whatever was the theory, at the end there is an activity of those anaesthetic agents which is produced on the cellular levels normally, which acts basically on the synaptic transmission & as we all now, the synaptic transmission is the basic process in which the neurotransmiters will be sent from one nervous axon to the other & through this mechanism we’ll feel the pain coming from the peripheral nervous system & reaching the brain to be translated as pain, so anaesthetics works by interupting this transmission in a way or other which helps reducing or cancelling the sensation of the pain at a particular time
So the effects on the axonal conduction process is considered to be a critical part in the practice of anaesthesia on patients, so the inhibition of this synaptic conduction process can be acheived in different mechanisms including the following
A) By decreasing the neurotransmitter release process
B) By the inhibition of the action of the neurotransmitter
C) By the reduction of the excitibility of the postsynaptic cell
B) By the inhibition of the action of the neurotransmitter
C) By the reduction of the excitibility of the postsynaptic cell
Through the past mentioned mechanisms, the reduction in the transmitter release & \ or the reduction in the excitibility of the postsynaptic cell are the most studied kinds & the most acceptable ways on actual clinical studies
For example, the reduction of Acetylcholine release was shown & proved in some peripheral nerves, at the same time, a decrease in the postsynaptic sensitivity had been shown in both central & peripheral nervous system studies & this decrease in the sensitivity was due to the inhibition process of the ligan-gated ion channels there, & this last process "the decrease in the postsynaptic sensitivity" was shown for example with BARBITURATES, in which they enhanced the low sensitivity process in these areas & at the same time this effect was occuring also with some volatile anaesthetics
Studies also were done to understand the exact region in the brain which was responsible for the anaesthetics action & these studies showed in a way or another that the THALAMIC SENSORY RELAY NUCLEI & THE DEEP LAYER OF THE CORTEX TO WHICH THESE NUCLEI PROJECT were the most sensitive areas working along with the anaesthetics, this area includes the routes taken by the sensory impulses to reach the cortex, so the general idea is presented by inhibiting this transmission & inhibiting the sensory impulses from reaching the cortex through this route, which means at the end that the brain will not receive the impulse & will not generate the feeling of PAIN at the end, another theory which enhance our awareness about the brain function is that anaesthesia even in small concentrations causes a mild AMNESIA effects on the patients, this is due to the interference which happens between the anaesthetic agent & the hippocampal functions & it is known that the hippocampus is the responsible for the short-term memory functions, thats’ why mild experiences with the anaesthesia can’t be exactly & directly remembered by the patient even if with small doses of the anaesthetic agent
And as the anaesthesia dose increase, the brain functions as a whole organ will be effected tissue by tissue, including the motor control & the reflex activities, the respiration & the autonomic regulations, so at the end & while increasing the dose of the anaesthsia, we can’t exactly describe a specific site in which the anaesthetic agent will work on it
BRIEF
Briefly we can say & as a continuing to the past lecture that there are evidences showing & describing the general actions of the anaesthesia, in which it have to be lipid & protein soluble to some extends, it will effects the cell structure & walls & will effect the conduction mechanism in them, through decreasing the release of neurotransmitter & through enhancing the decrease in the sensitivity of the postsynaptic cells, it will exert its’ effects
In smaller doses it will cause amnesia & effect the hippocampal functions & by increasing the dose it will start effecting all the brain as a general whole organ making it more difficult to predict the exact location of its pharmacological actions
TO BE CONTINUED
To read the first parts of the older lectures please press on the following URL address
General Anaesthetic Agents Part I
mortada8.maktoobblog.com/1537329/%D8%A7%D9%84%D8%AA%D8%AE%D8%AF%D9%8A%D8%B1-%D8%A7%D9%84%D8%B9%D8%A7%D9%85-%D9%88%D8%A7%D9%84%D9%85%D9%88%D8%A7%D8%AF-%D8%A7%D9%84%D9%85%D8%AE%D8%AF%D8%B1%D8%A9general-anaesthetic-
المزيدmortada8.maktoobblog.com/1537329/%D8%A7%D9%84%D8%AA%D8%AE%D8%AF%D9%8A%D8%B1-%D8%A7%D9%84%D8%B9%D8%A7%D9%85-%D9%88%D8%A7%D9%84%D9%85%D9%88%D8%A7%D8%AF-%D8%A7%D9%84%D9%85%D8%AE%D8%AF%D8%B1%D8%A9general-anaesthetic-
هل أستخدم مادة كارديو تونيك بلس أو لا أستخدمها؟
نوفمبر 22nd, 2009 كتبها اسماعيل العبد مرتضى نشر في , Clinical Pharmacology & Therapeutics, Drugs & Supplements, General Medical Articles,هل أستخدم مادة كارديو تونيك بلس أو لا أستخدمها؟
سؤال موجه على الإيميل من أحد القراء
=-=-=-=-=-=-=-=-=-=-=-=-=-=-=-
From: …………..@hotmail.com
To: mortada8@hotmail.com
Subject: RE:
Date: Sat, 21 Nov 2009 17:54:46 +0200
To: mortada8@hotmail.com
Subject: RE:
Date: Sat, 21 Nov 2009 17:54:46 +0200
اخى الكريم او ابنى الكريم ان كنت تقبلها فانا عمرى ستون عاما
واكبر ابنائى مهندس جرافيك عمره 31 عاما
عموما
زرت مدونتك ورأيت أنها مدونة متخصصة رائعه
فاوحت لى تلك الزياره بسؤال لواحد من المتخصصين فى الصيدله وهو :
ما تقييمك لدواء مرضى القلب المسمى كورديو تونيك بلس ؟
وهل هو فعال بالشكل الذى يوصف به ام ان هناك مبالغات ؟
تحياتى لك للعلم أنا أيضا لى مدونه اسمها…………………………………
=-=-=-=-=-=-=-=-=-=-=-=-=-=-=-
تحياتي سيد ………………………..
لا يوجد مشكلة بالنسبة للألقاب…كل الناس خير وبركة
بالنسبة للمدونة أشكرك على مجاملتك المقبولة…وبالنسبة لمدونتك فأنا أعرفها صديقي المحترم من زمان..فانا متابع عام أحيانا من هنا وهناك
المهم أدخل في الموضوع الأهم بالنسبة لي وهو سؤالك عن المادة
أولا هي ليست بدواء ولكنها "عقار" وهذا يختلف طبيا حيث أن العقار يكون مكون من مواد طبيعية بشكل أساسي, أي أن المادة الفعالة به تكون مادة طبيعية إما عشبية أو ما شابه, أو مادة مستخرجة من الطبيعة بحيث لا يتكون من مواد "مخلقة" أو مصنعة كيميائيا ولكني وبنفس الوقت إطلعت على مكونات هذا العقار ووجدت التالي كرأي شخصي
أولا إنه يتكون من مواد طبيعية
ثانيا أنه يتكون من مجموعة من الأعشاب, بعضها معترف به طبيا وصيدلانيا على أنه يعمل كذا وكذا ويساعد في عمل كذا وكذا أي بمعنى أن العشبة خضعت للدراسات السريرية ومفعولها معلوم
ثالثا أن بعض المكونات ليست بالمكونات المتعارف عليها بشكل كبير طبيا ولم تخضع بشكل كافي للدراسات السريرية وليست تصنف بشكل مباشر تحت تصنيف العقاقير المعروفة
رابعا .. وبسبب تلك النقاط الماضية فأنا لا أستطيع أن أحكم على مفعوله بشكل كامل حيث أنه غير معروف بشكل كامل التركيب أو المفعول الطبي, ولكني أستطيع أن أقول أنه لا مانع من استخدامه إذا كان الشخض المستخدم يحاول حماية نفسه من مشاكل القلب العامة كارتفاع ضغط الدم أو ما الى ذلك, على أن يتم استخدامه بعدم التزامن مع أي أدوية أخرى وعلى أن يكون الشخص لا يعاني من أي أعراض أخرى عامة قبل إخبار الصيدلي أو الطبيب المسؤول
خامسا: أنه لا يستخدم بشكل مباشر مع مرضى القلب على أنه علاج بديل للعلاجات الطبية المعروفة
المزيدلا يوجد مشكلة بالنسبة للألقاب…كل الناس خير وبركة
بالنسبة للمدونة أشكرك على مجاملتك المقبولة…وبالنسبة لمدونتك فأنا أعرفها صديقي المحترم من زمان..فانا متابع عام أحيانا من هنا وهناك
المهم أدخل في الموضوع الأهم بالنسبة لي وهو سؤالك عن المادة
أولا هي ليست بدواء ولكنها "عقار" وهذا يختلف طبيا حيث أن العقار يكون مكون من مواد طبيعية بشكل أساسي, أي أن المادة الفعالة به تكون مادة طبيعية إما عشبية أو ما شابه, أو مادة مستخرجة من الطبيعة بحيث لا يتكون من مواد "مخلقة" أو مصنعة كيميائيا ولكني وبنفس الوقت إطلعت على مكونات هذا العقار ووجدت التالي كرأي شخصي
أولا إنه يتكون من مواد طبيعية
ثانيا أنه يتكون من مجموعة من الأعشاب, بعضها معترف به طبيا وصيدلانيا على أنه يعمل كذا وكذا ويساعد في عمل كذا وكذا أي بمعنى أن العشبة خضعت للدراسات السريرية ومفعولها معلوم
ثالثا أن بعض المكونات ليست بالمكونات المتعارف عليها بشكل كبير طبيا ولم تخضع بشكل كافي للدراسات السريرية وليست تصنف بشكل مباشر تحت تصنيف العقاقير المعروفة
رابعا .. وبسبب تلك النقاط الماضية فأنا لا أستطيع أن أحكم على مفعوله بشكل كامل حيث أنه غير معروف بشكل كامل التركيب أو المفعول الطبي, ولكني أستطيع أن أقول أنه لا مانع من استخدامه إذا كان الشخض المستخدم يحاول حماية نفسه من مشاكل القلب العامة كارتفاع ضغط الدم أو ما الى ذلك, على أن يتم استخدامه بعدم التزامن مع أي أدوية أخرى وعلى أن يكون الشخص لا يعاني من أي أعراض أخرى عامة قبل إخبار الصيدلي أو الطبيب المسؤول
خامسا: أنه لا يستخدم بشكل مباشر مع مرضى القلب على أنه علاج بديل للعلاجات الطبية المعروفة
Interaction between Morphine & Nalorphine
نوفمبر 18th, 2009 كتبها اسماعيل العبد مرتضى نشر في , Biopharmaceutical studies, Clinical Pharmacology & Therapeutics, Drugs & Supplements, General Medical Articles, Medicinal Chemistry, Pharmacokinetics,Interaction between Morphine & Nalorphine
A question received to my personal email via a reader
A question received to my personal email via a reader
التفاعل ما بين مادة المورفين والنالورفين
سؤال موجه من أحد القراء على الإيميل
سؤال موجه من أحد القراء على الإيميل
The reply is available in both arabic & english Languages
الإجابة موجودة باللغتين العربية والإنجليزية
الإجابة موجودة باللغتين العربية والإنجليزية
=-=-=-=-=-=-=-=-=-=-=-=-=-=-=-
| Wed, 18 Nov 2009 15:57:10 | |||
| من: |
| ||
| الى: |
| ||
| الموضوع: | drug antagonism morphine&analorphine |
اريد رد رجااااءا وبسرعة حول التداخلات الدوائية المذكورة
| "لا يتحمّل مكتوب أيّة مسؤوليّة عن المواد الّتي يتم عرضها أو نشرها في مدوّنات مكتوب. ويتحمل المستخدمون بالتالي كامل المسؤولية عن كتاباتهم وإدرجاتهم التي تخالف القوانين أو تنتهك حقوق الملكيّة أو حقوق الآخرين أو أي طرف آخر. " |
Maktoob.com Inc.
Samsung Building EIB-03, DIC
Dubai, UAE
Tel: +97143913640
Samsung Building EIB-03, DIC
Dubai, UAE
Tel: +97143913640
This message was sent to mortada8@maktoob.com
pmguid:mortada8@maktoob.com blogs
pmguid:mortada8@maktoob.com blogs
=-=-=-=-=-=-=-=-=-=-=-=-=-=-=-
Morphine is a kind of Opioid analgesic, Nalorphine is another kind also of milder opioid analgesics
Now the point is that morphine is a strong kind, but on the other hand NALORPHINE is considered to be a COMPETITIVE ANATGONIST which means that nalorphine action will be depending on the concentration given to the patient, it works on different kinds of receptors & it will have different kinds of actions, but before speaking about them, let me please explain for you the idea of competitive anatgonism in medical studies
Now the point is that morphine is a strong kind, but on the other hand NALORPHINE is considered to be a COMPETITIVE ANATGONIST which means that nalorphine action will be depending on the concentration given to the patient, it works on different kinds of receptors & it will have different kinds of actions, but before speaking about them, let me please explain for you the idea of competitive anatgonism in medical studies
When we say competitive antagonist, this means that the drug molecule have a structure which is similar to some extend to the targeted receptor, so when 2 drugs are given at the same time, one of them is a competitive antagonist to the other, that means that the antagonist will start competing for the targeted receptors with the original drug
This means that instead of the drug being attached to the receptors to exert a medical & pharmacological action, you’ll find that some parts of the other drug "the antagonist" are already attached, & that’s why the pharmacological action of the original drug "for example morphine" will decrease, because the morphine will not find place enough to attach to enough receptors to exert the normal pharmacological action
Now you have to consider different points which are that first of all this doesn’t mean that morphine will not have an action, but it means that the action will be less then before
If you increased the dose of morphine, this will overcome the antagonistic action of nalorphine, since it is COMPETITIVE, which means that it is dose dependent,
المزيدالتخدير العام والمواد المخدرة……General Anaesthetic Agents
أكتوبر 17th, 2009 كتبها اسماعيل العبد مرتضى نشر في , Clinical Pharmacology & Therapeutics, Drugs & Supplements, Pharmacokinetics,التخدير العام والمواد المخدرة
General Anaesthetic Agents
General Anaesthetic Agents
محاضرة متخصصة تابعة لقسم الفارماكولوجي السريري وعلوم الأدوية
Specialized Lecture in Cinical Pharmacology
متوفرة باللغتين العربية والإنجليزية
Available in both languages, Arabic & English
مناقشة إسماعيل مرتضى Discussed by Ismail Mortada
Specialized Lecture in Cinical Pharmacology
متوفرة باللغتين العربية والإنجليزية
Available in both languages, Arabic & English
مناقشة إسماعيل مرتضى Discussed by Ismail Mortada

Aneasthetics compose a large section & a huge importance in the medical field, since they are very necessary for surgeries to be done successfully & for operations to run smoothly & without pain, that’s why studying them extensively is important so that to be able to go further more later on in discovering new agents with lower side effects & more efficiency , & they are (anaesthetics) divided into 2 major types which are as the following
A) Local Anaesthetics
B) General Anaesthetics
A) Local Anaesthetics
B) General Anaesthetics
And in this lecture & the coming parts & episodes of it, I’m going to discuss & revise GENERAL ANESTHETICS from Clinical point of view & from Pharmacological point of view depending basically on hard medical books & references + my personal old university lecture notes
=-=-=-=-=-=-=-=-=-=-=-=-=-=-=-=-=-=-=-=-=-=-=
Physiochemical Theories of Anaesthesia
Unlike most of the other drugs in pharmacology, General Anaesthetic agents are not exactly & totally understood from pharmacological mechanism of action point of view until now, since they have different chemical structures & electronic configuration -anaesthetic agents- so they are not belonging to any basic single chemical class, the pharmacological action of general aneasthetics requires basically a specific uniimportant physiochemical properties, those agents lacks an exact RECEPTOR which they work in & they have a low profile in chemical specificity regarding this matter
They appear to act principally on the cells membranes & the theories of anaesthesia focuses on the interactions with the 2 major components of the cell membrane which are the lipids & proteins, That’s why General Anaesthesia Theories would be divided into 2 major sections which are as the following
A) The Lipid Theory
B) The Protein Theory
A) The Lipid Theory
B) The Protein Theory
Note also that there are another theories available in the scientific field but I concentrated on those 2 major ones since they are the basic original theories mentioned in pharmacology references & were taught to us before
=-=-=-=-=-=-=-=-=-=-=-=-=-=-=-=-=-=-=-=-=-=-=
A) THE LIPID THEORY
The Lipid Theory is based on the idea that there is a close correlation between the Anaesthetic Potency & the Lipid Solubility of the agent, & it believes that Narcosis commences (Narcosis means exactly the privation of sense & consiousness due to using a nracotic agent) when any chemically indifferent substances has attained a certain molar concentration in the lipids of the cells, so the agent must be lipid soluble & to reach a specific molar concentration, when those 2 factors occurs, the anaesthetic affect will start also
Now in general and before going deeper into this particular theory, it is well known in the medical field that for a substance in general to be able to pass the cell membranes, it needs to be holding a special percentage of lipid solubility so that to pass the LIPID membranes of the living cells in general, for sure there are other mechanisms of excerting actions on the cells other than being only lipid soluble, but still lipid solubility plays the major role in this reaction & this is why the LIPID THEORY is a logical theory which depends on a basic scientific evidence
The relationship between anaesthetic activity & lipid solubility has been repeatedly confirmed, see the following diagram which shows results obtained in humans where the Minimal Alveolar Concentration (MAC) which is inversely proportional to potency required to produce a lack of response to painful stimulation is plotted against lipid solubility

Please Press on the picture to enlarge it & read the content clearly
It is expressed as oil : water partition coeffiecient (the past diagram shows oil in gas partition & it is the saem concept since I couldn’t find the exact diagram that I want), for a wide range of inhalation anaesthetics, This diagram is called the Overton-Meyer studies & it did not suggest any particular mechanism of action, but it showed a basic interesting correlation which any theory of anaesthetics needs to take in account in general, the oil : water partition should predict the partition into membrane lipids, while the keeping the old agreement that anaethesia make an alteration in the membrane function
Now the right question would be that HOW might the introduction of an inert new substance molecules into the cell membranes causes a full disturbance in those cells & causes a clear functional disturbance & changes? To answer this questions there are different ideas, in which one of them is called "The pressure reversal anaesthesia theory" which indicates that the "Volume Expansion" is the reason of those past mentioned effects, In animals such as newts, they are immobilised by the addition of an anaesthetic agent to the water, then the application of hydrostatic pressure to about 100 atmospheres immediately restores their mobility & the anaesthesia returns as soon as the pressure is lowered
Those results are compatible with the theory that anaesthesia occurs when volume of the lipid phase is expanded by about 0.4% as a result of the intrusion of anaesthetic molecules, Pressure is though to act simply by opposing this volume expansion, further work decreased also the doubt regarding this point of view
Another theory involves the increase in membrane fluidity due to the disorder that occurs in the packing array of membrane phospholipids, all the physiochemical measurments confirms that this happens, so, relatively high concentrations of the anaesthetic agents is needed & the affects are small by comparison with those of a modest (<1 degree C) rise in temperature, so also the relation directly between this theory & the pharmacological action is not exactly clear
=-=-=-=-=-=-=-=-=-=-=-=-=-=-=-
B) THE PROTEIN THEORY
Anaesthetics can bind to proteins as well as lipids, studies done on some kind of "enzymes" which means some kinds of proteins showed that there is a parallel relation between the action of enzyme inhibition & the anaesthetic agents functions, there were another evidences of relation between anaesthetic actions and the interaction with the functional membrane proteins, for example ligand-gated ion channels, A lot of anaesthetic agents at a concentration reached to cause anaesthesia had shown to inhibit the functions of excitatory receptors "like ionotropic glutamate acetylcholine or 5-HT receptors" as well as enhancing the inhibitory receptors functions "like GABA A & Glycine", the studies after that done on genetically engineered receptors showed that the effects depends on the presence of a particular domains in the receptor protein, which comprise specific "Modulatory sites"throug which the anaesthetic drugs exerts their effects on channel functions, there must be further studies done to clearify this effect and the past mentioned points, especially those experiments done on mice
From holding a moderate middle level of understanding both theories the lipid & the protein theory is athe basic view that the anaesthetics concentration at the lipid-protein interface within the cells membranes is important for the pharmacological action to occur & we have to keep in mind that most proteins have different or multi-functional reactions which will include more than one theory as a must
TO BE CONTINUED
=-=-=-=-=-=-=-=-=-=-=-=-=-=-=-
=-=-=-=-=-=-=-=-=-=-=-=-=-=-=-
=-=-=-=-=-=-=-=-=-=-=-=-=-=-=-
=-=-=-=-=-=-=-=-=-=-=-=-=-=-=-
=-=-=-=-=-=-=-=-=-=-=-=-=-=-=-
التخدير العام والمواد المخدرة
General Anaesthetic A
المزيدGeneral Anaesthetic A
الفرق بين الحقيقة والخيال
سبتمبر 24th, 2009 كتبها اسماعيل العبد مرتضى نشر في , Clinical Pharmacology & Therapeutics, Drugs & Supplements, General Medical Articles,الفرق بين الحقيقة والخيال
مقالة طبية عامة
فارماكولوجي وعلوم أدوية, قسم الصيدلة السريرية
مناقشة إسماعيل مرتضى
مقالة طبية عامة
فارماكولوجي وعلوم أدوية, قسم الصيدلة السريرية
مناقشة إسماعيل مرتضى

وددت كثيرا لو توقفت للحظة وقلت للجميع, أرجوكم, لا تصدقوني تماما, مع أني صادق, ولكن ليس كل ما يلمع ذهبا, فإن الذين يعرفون لا يستوون بالذين لا يعرفون (لا أقصد نفسي بالمعرفة) ولكن هذه هي الحقيقة وهذا هو الواقع الذي لابد أن يتحدث به احدهم يوما ما
أتحدث هنا عن الأدوية بشكل عام, وعن العقاقير ومستحضرات الإستخلاص الطبيعي بشكل خاص, وعن العلاجات بكل أنواعها على وجه التعميم
=-=-=-=-=-=-=-=-=–=-=-=-=-=-=-=
حقيقة ما اود قوله وباختصار هو ان من ينكر أن الأدوية هي إكتشاف مذهل وهي منتوجة تعب مضني وشاق وتفكير وتحليل وتجربة وقياس منطقي مرعب, فهو كمن ينكر الشمس في وضح النهار أو كمن ينكر على نفسه حقه بالحياة, وقد واجهت في حياتي العملية الكثيرين ممن ينكروا أمور كهذه, ومع أني أجد الكثير من الأعذار لعامة الناس والغير متخصصين بظنونهم تلك, إلا أنني أطلب منهم التوقف والتفكير للحظة فيما يقولون, فمن يستطيع إنكار مفعول البنج في غرفة العمليات؟ ومن يستطيع إنكار مفعول حبة مورفين لمريض متألم؟ ومن يستطيع إنكار مفعول سيجارة على شخص يحبها؟ أم من يستطيع أن ينكر مفعول الحشيش على الحشاشيين؟أليست كلها مواد كيميائية؟ وهي كلها تصنف لدينا بتصنيفات دقيقة ومتخصصة؟
ولكني سأقول لكم ما هو الفرق الحقيقي بين الدواء وبين الهباء… وبين الحقيقة وبين الخيال
الحقيقة متمثلة بوجود مادة كيميائية, لها شكلها المدروس, ولها تشريحها الواضح, ولها خصائصها الكيميائية والفيزيائية والتي لا نستطيع التخلي عن التفكير بها, والحقيقة هي أن أي شيء يدخل الى جسم الإنسان -أو أي كائن حي آخر- فإنه سيتفاعل ويتأثر ويؤثر في هذا الجسم, تبعا لخصائص هذه المادة وتبعا لنوعية هذا الجسم, ولا يوجد على سبيل الإطلاق مادة تدخل دون حدوث تفاعل, حتى تلك الأدوية المزيفة التي تعطى للمرضى في حدائق التجارب المخبرية في المستشفى, لا تلبث إلا أن تحدث تفاعل (فعدم حدوث تفاعل أصلا يعتبر نوع من أنواع التفاعلات من وجهة نظر الكيمياء البحتة حيث أنه يلغي أو يؤثر ولو بنسبة ضئيلة
المزيد
Clarinase
يوليو 6th, 2009 كتبها اسماعيل العبد مرتضى نشر في , Clinical Pharmacology & Therapeutics, Drugs & Supplements, Comments Off ,Drugs & Supplements
Clarinase
Clarinase
The Informations are taken from the leaflet supplied with the drug itself
المعلومات مأخوذة من النشرة الدوائية المرافقة للدواء نفسه
Don’t use any supplement or medication without referring to the Physician or Pharmacsit, they are the experts who can help you to manage your medication use
الرجاء عدم استخدام أي دواء قبل مراجعة الطبيب أو الصيدلي, لأنهم الخبراء المسؤولون عن إبداء التعاون والنصيحة الصحيحة فيما يخص تناولك للأدوية ولحالتك الصحية بشكل عام
أخوكم إسماعيل المرتضى

It’s a brand of Loratadine & Pseudoephedrine sulfate
Long acting \ Non-Sedating Antihistamine \ Decongestant Tablets
Long acting \ Non-Sedating Antihistamine \ Decongestant Tablets
DESCRIPTION: Each clarinase repetab tablets contains 5mg loratadine in the tablet coating and 120mg pseudoephedrine sulfate equally distributed between the tablet coating and the barrier-coated core. The 2 active components in the coating are quickly liberated; release of the decongestant in the core is delayed for several hours
Inactive Ingredients: maize starch, povidone, magnesium stearate & purified water
ACTIONS: Loratadine is a potent long acting tricyclic antihistamine with peripheral H1-receptor antagonistic activity, Pseudoephedrine sulfate, one of the naturally occuring alkaloids of ephedra and an orally administered vasoconstrictor, produce a gradual but sustained decongestant effect facilitating shrinkage of congested mucosa in upper respiratory areas, The mucus membrane of the respiratory tract is decongested through the action on the sympathetic nerves
INDICATIONS & USAGE: Clarinase repetabs tablets are indicated for the relief of symptoms associated with allergic rhinitis and the common cold including nasal congestion, sneezing, rhinorrhea, pruritus & lacrimation, Clarinase repetabs tablets are recommended when both the antihistaminic properties of loratadine and the decongestant effect of pseudoephedrine sulfate are desired
DOSAGE & ADMINSTIRATION: Adults & children 12 years of age and over; one Clarinsae repetab tablet twice a day
المزيدDifferin
يونيو 19th, 2009 كتبها اسماعيل العبد مرتضى نشر في , Clinical Pharmacology & Therapeutics, Drugs & Supplements,Drugs & Supplements
Differin
Differin
The Informations are taken from the leaflet supplied with the drug itself
المعلومات مأخوذة من النشرة الدوائية المرافقة للدواء نفسه
Don’t use any supplement or medication without referring to the Physician or Pharmacsit, they are the experts who can help you to manage your medication use
الرجاء عدم استخدام أي دواء قبل مراجعة الطبيب أو الصيدلي, لأنهم الخبراء المسؤولون عن إبداء التعاون والنصيحة الصحيحة فيما يخص تناولك للأدوية ولحالتك الصحية بشكل عام
Translated to Arabic مترجم للعربية
أخوكم إسماعيل المرتضى

Patient information leaflet
Please read this leaflet carefully before you start to use DIFFERIN, Don’t throw this leaflet away, You might want to read it again while using DIFFERIN
This leaflet has been prepared to help you use this medicine correctly, However, this leaflet does not tell you everything about your medicine, so if you have any questions please ask your doctor
Please read this leaflet carefully before you start to use DIFFERIN, Don’t throw this leaflet away, You might want to read it again while using DIFFERIN
This leaflet has been prepared to help you use this medicine correctly, However, this leaflet does not tell you everything about your medicine, so if you have any questions please ask your doctor
What is in your Differin
The name of your medicine is Differin
Differin cream contains the active ingredient adapalene 0.1% and also contains carbomer 934p, PEG-20 methyl glucose sesquistearate, glycerol (E422), natural squalene, methyl parahydroxybenzoate (E218)< propyl parahydroxybenzoate (E216), disodium edetate, methyl glucose sesquistearate, phenoxyethanol, cyclomethicone, sodium hydroxice and purified water
Differin gel contains adapalene 0.1%, carbomer 940, propylene glycol, poloxamer 182, phenoxyethanol, disodium edetate, methyl parahydroxybenzoate, sodium hydroxide, purified water
The name of your medicine is Differin
Differin cream contains the active ingredient adapalene 0.1% and also contains carbomer 934p, PEG-20 methyl glucose sesquistearate, glycerol (E422), natural squalene, methyl parahydroxybenzoate (E218)< propyl parahydroxybenzoate (E216), disodium edetate, methyl glucose sesquistearate, phenoxyethanol, cyclomethicone, sodium hydroxice and purified water
Differin gel contains adapalene 0.1%, carbomer 940, propylene glycol, poloxamer 182, phenoxyethanol, disodium edetate, methyl parahydroxybenzoate, sodium hydroxide, purified water
What does Differin do
A) The active ingredient in Differin is adapalene which has Anti-Inflammatory effect reducing soreness and irritation
B) It is used on the face, chest or back for acne, where the skin have lots of blackheads, spots & pimples
C) Adapalene is only absorbed into the body in a very small amounts, and has little effects, except on the surface of the skin
A) The active ingredient in Differin is adapalene which has Anti-Inflammatory effect reducing soreness and irritation
B) It is used on the face, chest or back for acne, where the skin have lots of blackheads, spots & pimples
C) Adapalene is only absorbed into the body in a very small amounts, and has little effects, except on the surface of the skin
Advice: When using Differin for the first time
If you answer yes to any of the following questions, or are not sure, talk to your doctor before using this medicine
A) Have you had a reaction to Differin or any of its ingredients? Please check by reading the list of ingredients above
B) Are you or could you be pregnant
If you answer yes to any of the following questions, or are not sure, talk to your doctor before using this medicine
A) Have you had a reaction to Differin or any of its ingredients? Please check by reading the list of ingredients above
B) Are you or could you be pregnant
What to avoid when using Differin
A) Don’t apply Differin to your chest, if you are breast feeding
B) Don’t use this product for children
C) Don’t use Differin on areas where you have cuts or scrapes
A) Don’t apply Differin to your chest, if you are breast feeding
B) Don’t use this product for children
C) Don’t use Differin on areas where you have cuts or scrapes
Helpful advice when using Differin
A) When using Differin on the face, don’t get it into your eyes, mouth and angles of the nose & avoid other very sensitive areas of your body
B) Other acne products (containing benzoyl peroxide, erythromycin or clindamycin), maybe used with Differin, but they MUST be applyed in the morning & Differin at night
C) Cosmetics maybe used but they must be non-comedogenic and non-astringent; for example they should not cause blackheads or dry the skin
D) Using more than the recommended amount of Differin may result in very red & sore skin
E) Differin is best applyed to your skin after washing and drying
F) If you are using any medicines make sure you tell your doctor
A) When using Differin on the face, don’t get it into your eyes, mouth and angles of the nose & avoid other very sensitive areas of your body
B) Other acne products (containing benzoyl peroxide, erythromycin or clindamycin), maybe used with Differin, but they MUST be applyed in the morning & Differin at night
C) Cosmetics maybe used but they must be non-comedogenic and non-astringent; for example they should not cause blackheads or dry the skin
D) Using more than the recommended amount of Differin may result in very red & sore skin
E) Differin is best applyed to your skin after washing and drying
F) If you are using any medicines make sure you tell your doctor
How to use Differin
A) Differin is applied at night before going to bed, unless your doctor has told you otherwise
B) Throughly wash the areas to be treated with water, make sure the skin is clean and dry before using Differin
C) Put a thin film of Differin with your fingertips on the affected areas and rub it gently
D) Do not forget to wash your hands afterwards
E) How long will you have to use Differin depends on how quickly your acne improves, After you have used Differin for 3 months, It is imporant that you see your doctor. He\she can then check the improvement of your acne
F) Don’t worry if your forget to apply your Differin at night time, When you remember, start using it again, in the same way as before
A) Differin is applied at night before going to bed, unless your doctor has told you otherwise
B) Throughly wash the areas to be treated with water, make sure the skin is clean and dry before using Differin
C) Put a thin film of Differin with your fingertips on the affected areas and rub it gently
D) Do not forget to wash your hands afterwards
E) How long will you have to use Differin depends on how quickly your acne improves, After you have used Differin for 3 months, It is imporant that you see your doctor. He\she can then check the improvement of your acne
F) Don’t worry if your forget to apply your Differin at night time, When you remember, start using it again, in the same way as before
While you are using Differin
Like many medicines Differin may occasionally cause un-wanted effects, such as irritation of the skin, Occasionally stinging at the application site maybe experienced
A) If you have any of these or any other unusual effects, and they are bad enough to trouble you, consult your doctor
B) If you experience sensitivity or irritation when applying Differin, stop is and tell your doctor, you maybe asked to use it less often, or to stop using for a short time
C) If you follow the instructions for use, it should not be possible to use too much or overdose, If, in the rare event that Differin is accidentally swallowed, you should seek medical advice
Like many medicines Differin may occasionally cause un-wanted effects, such as irritation of the skin, Occasionally stinging at the application site maybe experienced
A) If you have any of these or any other unusual effects, and they are bad enough to trouble you, consult your doctor
B) If you experience sensitivity or irritation when applying Differin, stop is and tell your doctor, you maybe asked to use it less often, or to stop using for a short time
C) If you follow the instructions for use, it should not be possible to use too much or overdose, If, in the rare event that Differin is accidentally swallowed, you should seek medical advice
How to store your Differin
Keep your Differin in a safe place where children cannot see or reach it, your medicine could harm them
Keep the medicine at normal room temperature (below 25 degree’s) and do not use if it is out of date
Keep your Differin in a safe place where children cannot see or reach it, your medicine could harm them
Keep the medicine at normal room temperature (below 25 degree’s) and do not use if it is out of date
Further Information
A) Always keep your medicine in a safe place out of sight and reach of children
B) Further information is available from your doctor
A) Always keep your medicine in a safe place out of sight and reach of children
B) Further information is available from your doctor
LABORATORIES GLADERMA
Z.I. - MONTDESIR
74540 Alby-sur-Cheran
France
Z.I. - MONTDESIR
74540 Alby-sur-Cheran
France
Gladerma International
Tour Europlaza - La Defence 4
20, avenue Andre Prothin
92927 La Defence Cedex
France
Tour Europlaza - La Defence 4
20, avenue Andre Prothin
92927 La Defence Cedex
France
=======================================
ديفرين
أدابالين جل 0.1%
النشرة الطبية للمريض
أدابالين جل 0.1%
النشرة الطبية للمريض
من فضلك اقرأ هذه النشرة بعناية قبل استخدام ديفرين واحتفظ بها فربما تريد الاطلاع عليها مرة أخرى أثناء استخدامك للمستحضر
سوف تساعدك هذه النشرة على استخدام الدواء بالطريقة الصحيحة, وحيث انها لا تحتوي على كل المعلومات الطبية لذا يرجى استشارة الطبيب عندما يوجد أي استفسار
سوف تساعدك هذه النشرة على استخدام الدواء بالطريقة الصحيحة, وحيث انها لا تحتوي على كل المعلومات الطبية لذا يرجى استشارة الطبيب عندما يوجد أي استفسار
ما هو ديفرين
ديفرين هو الاسم التجاري لهذا الدواء
يحتوي ديفرين كريم على مادة فعالة وهي أدابالين 0.1% كما يحتوي على كاربومر 934 بي, بي اي جي-20 ميثيل جلوكوز سيسكويستيرات, جليسرول اي 422, سكوالين طبيعي, مثيل باراهيدروكسي بنزوات اي216, بروبيل باراهيدروكسي بنزوات اي216, اديتات ثنائي الصوديوم, ميثيل جلوكوز سيسكويستيرات, فينوكسي ايثانول, سيكلوميثيكون, هيدروكسيد الصوديوم وماء نقي
يحتوي ديفرين جل 0.1% على مادة فعالة هي ادابالين,
المزيدديفرين هو الاسم التجاري لهذا الدواء
يحتوي ديفرين كريم على مادة فعالة وهي أدابالين 0.1% كما يحتوي على كاربومر 934 بي, بي اي جي-20 ميثيل جلوكوز سيسكويستيرات, جليسرول اي 422, سكوالين طبيعي, مثيل باراهيدروكسي بنزوات اي216, بروبيل باراهيدروكسي بنزوات اي216, اديتات ثنائي الصوديوم, ميثيل جلوكوز سيسكويستيرات, فينوكسي ايثانول, سيكلوميثيكون, هيدروكسيد الصوديوم وماء نقي
يحتوي ديفرين جل 0.1% على مادة فعالة هي ادابالين,
Retin-A Cream
مايو 29th, 2009 كتبها اسماعيل العبد مرتضى نشر في , Clinical Pharmacology & Therapeutics, Drugs & Supplements,Drugs & Supplements
Retin-A Cream
Retin-A Cream
The Informations are taken from the leaflet supplied with the drug itself
المعلومات مأخوذة من النشرة الدوائية المرافقة للدواء نفسه
Don’t use any supplement or medication without referring to the Physician or Pharmacsit, they are the experts who can help you to manage your medication use
الرجاء عدم استخدام أي دواء قبل مراجعة الطبيب أو الصيدلي, لأنهم الخبراء المسؤولون عن إبداء التعاون والنصيحة الصحيحة فيما يخص تناولك للأدوية ولحالتك الصحية بشكل عام
أخوكم إسماعيل المرتضى

Retin-A
For the topical treatment of Acne
For the topical treatment of Acne
Therapeutic class
Treatment of Acne
Treatment of Acne
Composition
Retin-A contains as active ingredient tretinoin (retinoic acid) and is presented in 3 different forms
Gel 0.01% or 0.025% tretinoin
Cream 0.025%, 0.05% or 0.1% tretinoin
Solution 0.1% tretinoin
Conserv: butylhydroxytoluol - cream - plus acid sorbinic and excip
Retin-A contains as active ingredient tretinoin (retinoic acid) and is presented in 3 different forms
Gel 0.01% or 0.025% tretinoin
Cream 0.025%, 0.05% or 0.1% tretinoin
Solution 0.1% tretinoin
Conserv: butylhydroxytoluol - cream - plus acid sorbinic and excip
Pharmacodynamic properties
Although th exact mode of action of tretinoin is unknown, current evidence suggest the effectiveness of tretinoin in acne is primarily due to its ability to modify abnormal follicular Keratinization, Acne comedones form in follicles with excessively Keratinized epithelial cells, The accumulation of keratinized material in the follicle initiate comedone formation
Tretinoin promotes detachment of cornified cells and enhanced shedding of corenocytes from the follicle, By increasing the mitotic activity of follicular epithelia, tretinoin also increases the turnover rate of thin, loosely, adherent corneocytes, Through these actions, tretinoin prevents the formation of microcomedo, The precursor region for acne vulgaris
Additionaly, tretinoin acts by modulating the proliferation and differentiation of skin cells, these effects are mediated by tretinoin’s interaction with a family of nuclear proteins, retinoic acid receptors
Activation of these nuclear receptors cause changes in the gene expression, which in turns, modify abnormal cellular processes, The exact mechanism whereby tertinoin-induced changes in gene expression regulate skin function are not understood
Although th exact mode of action of tretinoin is unknown, current evidence suggest the effectiveness of tretinoin in acne is primarily due to its ability to modify abnormal follicular Keratinization, Acne comedones form in follicles with excessively Keratinized epithelial cells, The accumulation of keratinized material in the follicle initiate comedone formation
Tretinoin promotes detachment of cornified cells and enhanced shedding of corenocytes from the follicle, By increasing the mitotic activity of follicular epithelia, tretinoin also increases the turnover rate of thin, loosely, adherent corneocytes, Through these actions, tretinoin prevents the formation of microcomedo, The precursor region for acne vulgaris
Additionaly, tretinoin acts by modulating the proliferation and differentiation of skin cells, these effects are mediated by tretinoin’s interaction with a family of nuclear proteins, retinoic acid receptors
Activation of these nuclear receptors cause changes in the gene expression, which in turns, modify abnormal cellular processes, The exact mechanism whereby tertinoin-induced changes in gene expression regulate skin function are not understood
Indication
Retin-A is indicated as topical therapy for the treatment of acne vulgaris
Retin-A is indicated as topical therapy for the treatment of acne vulgaris
Recommended Dosage
Adults
Retin-A should be applied once daily before retiring to the area of the skin where acne lesions occur, Only a sufficient quantity of medication should be applied to cover the affected areas lightly, using a gauze swab, cotton wool or the tips of clean finger, Over saturation should be avoided since excess medication could run into the eyes, angles of the nose, or other areas where treatment is not intended, Application of Retin-A may cause a transitory feeling of warmth or slight stinging
When administered according to recommended guidelines, Retin-A may produce a sligh erythema similar to that of mild sunburn, In cases where it is necessary to temorarily discontinue therapy or reduce the frequency of application, therapy should be resumed or the frequency of application increased when the patient becomes able to tolerate the treatment
Excess application of Retin-A does not provide more rapid or better results, In-fact, marked redness, peeling or discomfort may occur, If excess application accidentally or through over-enthusiastic use, Retin-A should be discontinued for several days before resumin therapy
Therapeutic effects maybe noticed after 2 to 3 weeks of use but more than 6 weeks of therapy maybe required before definite beneficial effects are seen
During the early weeks of treatment an apparaent exacerbation of inflammatory regions may occur, This is due to the action of medication on deep, previuosly unseen lesions and should not be considered to be a reason to discontinue therapy, Once a satisfactory response has been obtained, it maybe possible to maintain this improvement with less frequent application
Preior to treatment with Retin-A, areas to being treated should be throughly cleansed with water and a mild, non-medicated soap, The treated area should be washed no more than twice a day, after washing the skin should be dried gently & completely without rubbing it, areas of the skin being treated should be allowed to dry for atleast 20 to 30 minutes before application of Retin-A
Cosmetics& moisturizers maybe used during therapy with Retin-A, but the areas of the skin being treated should be washed throughly before Retin-A is applied, Astringent toiletries should be avoided
Adults
Retin-A should be applied once daily before retiring to the area of the skin where acne lesions occur, Only a sufficient quantity of medication should be applied to cover the affected areas lightly, using a gauze swab, cotton wool or the tips of clean finger, Over saturation should be avoided since excess medication could run into the eyes, angles of the nose, or other areas where treatment is not intended, Application of Retin-A may cause a transitory feeling of warmth or slight stinging
When administered according to recommended guidelines, Retin-A may produce a sligh erythema similar to that of mild sunburn, In cases where it is necessary to temorarily discontinue therapy or reduce the frequency of application, therapy should be resumed or the frequency of application increased when the patient becomes able to tolerate the treatment
Excess application of Retin-A does not provide more rapid or better results, In-fact, marked redness, peeling or discomfort may occur, If excess application accidentally or through over-enthusiastic use, Retin-A should be discontinued for several days before resumin therapy
Therapeutic effects maybe noticed after 2 to 3 weeks of use but more than 6 weeks of therapy maybe required before definite beneficial effects are seen
During the early weeks of treatment an apparaent exacerbation of inflammatory regions may occur, This is due to the action of medication on deep, previuosly unseen lesions and should not be considered to be a reason to discontinue therapy, Once a satisfactory response has been obtained, it maybe possible to maintain this improvement with less frequent application
Preior to treatment with Retin-A, areas to being treated should be throughly cleansed with water and a mild, non-medicated soap, The treated area should be washed no more than twice a day, after washing the skin should be dried gently & completely without rubbing it, areas of the skin being treated should be allowed to dry for atleast 20 to 30 minutes before application of Retin-A
Cosmetics& moisturizers maybe used during therapy with Retin-A, but the areas of the skin being treated should be washed throughly before Retin-A is applied, Astringent toiletries should be avoided
Contraindications
Hypersensitivity to any component of this product
Hypersensitivity to any component of this product
Warnings
General Precautions
In order to minimize the potential of additional skin irritation, care should be taken to avoid contact with the eyes, eyelids, angles of the nose, mouth, mucus membranes or other areas where treatment is not intended
Patients would be able to remove hair as usual (lucking, electrolysis, depilatories) but should avoid these procedures at night before applying Retin-A as they might result in skin irritation
Permanent wave solutions, waxingpreparations, medicated soaps & shampoos may sometimes irritate even normal skin, Caution should be used so that these products do not come into contact with skin treated with Retin-A
General Precautions
In order to minimize the potential of additional skin irritation, care should be taken to avoid contact with the eyes, eyelids, angles of the nose, mouth, mucus membranes or other areas where treatment is not intended
Patients would be able to remove hair as usual (lucking, electrolysis, depilatories) but should avoid these procedures at night before applying Retin-A as they might result in skin irritation
Permanent wave solutions, waxingpreparations, medicated soaps & shampoos may sometimes irritate even normal skin, Caution should be used so that these products do not come into contact with skin treated with Retin-A
Local Irritation
It is not recommended to initiate treatment with Retin-A or continue its use in the presence of skin irritation (erythema, peeling, pruritus, sunburn ..etc) until these symptoms subside
In certain sensitive individuals, Retin-A may induce severe local eryhtema, swelling, pruritus, warmth, burning or stinging, blistering, crusting and\or peeling at the site of the application, If the degree of local irritation warrants, the patient should be instructed to either apply the medication less frequently or discontinue its use temporarily
Trettinoin has been reported to cause severe irritation on eczematous skin and should be used with utmost caution in patients with this condition, If a patient experiences severe or persistence irritation, the patient should be advised to discontinue use of Retin-A completely, and if necessary, consult a physcian
Weather extremes such as wind, cold & low humidity maybe irritating to skin treated with Retin-A and may increase its dryness
It is not recommended to initiate treatment with Retin-A or continue its use in the presence of skin irritation (erythema, peeling, pruritus, sunburn ..etc) until these symptoms subside
In certain sensitive individuals, Retin-A may induce severe local eryhtema, swelling, pruritus, warmth, burning or stinging, blistering, crusting and\or peeling at the site of the application, If the degree of local irritation warrants, the patient should be instructed to either apply the medication less frequently or discontinue its use temporarily
Trettinoin has been reported to cause severe irritation on eczematous skin and should be used with utmost caution in patients with this condition, If a patient experiences severe or persistence irritation, the patient should be advised to discontinue use of Retin-A completely, and if necessary, consult a physcian
Weather extremes such as wind, cold & low humidity maybe irritating to skin treated with Retin-A and may increase its dryness
Exposure to sunlight
Exposure to sunlight, including ultraviolet sunlamps, may provoke additional irritation, Therefore, exposure should be avoided or minimized during the use of tretinoin, A patient experiencing considerable sun exposure tdue to occupational duties, or\and any patient inherently sensitive to the sun, should exercise particular caution, When exposure to sunlifght cannot be avoided, use of sunscreen products and protective clothing over treated areas is recommended
Exposure to sunlight, including ultraviolet sunlamps, may provoke additional irritation, Therefore, exposure should be avoided or minimized during the use of tretinoin, A patient experiencing considerable sun exposure tdue to occupational duties, or\and any patient inherently sensitive to the sun, should exercise particular caution, When exposure to sunlifght cannot be avoided, use of sunscreen products and protective clothing over treated areas is recommended
Children
Safety and effectiveness have not been established in children
Safety and effectiveness have not been established in children
Pregnancy & Lactation
Topical tretioin has not been shown to be teratogenic in Wistar Rats and rabbits when given in doses 1000 & 320 times the topical human dose, respectively, assuming that a 50Kg adult applies 250mg of 0.1% Retin-A topically, At these topical doses, however, a delayed ossification of several bones occured in rabbits, In rats, a dose dependent increase of supenumary ribs was observed, These changes are considered variants of normal development, The ossification changes are usually spontaneously corrected after weaning
There have been isolated reports of birth defects among babies born to women exposed to topical tertinoin during pregnancy , to date, there have been no adequate and well-controlled prospective studies performed in pregnant women and the teratogenic blood level of tretinoin is not known, However, a well-conducted retrospective cohort study of babies born to women exposed to topical tretinoin during the first trimester of pregnancy found no excess birth defects among these babies when compared with babies born to women in the same cohort who were not similarly exposed, topical tertinoin should be used during pregnancy only if the potential benefit justifies the potential risk to the fetus, it is not known wether tretinoin is excreted in the human milk, Since mny drugs are excreted in human milk, caution should be exrecised, When Retin-A is administered to a nursing mother
Topical tretioin has not been shown to be teratogenic in Wistar Rats and rabbits when given in doses 1000 & 320 times the topical human dose, respectively, assuming that a 50Kg adult applies 250mg of 0.1% Retin-A topically, At these topical doses, however, a delayed ossification of several bones occured in rabbits, In rats, a dose dependent increase of supenumary ribs was observed, These changes are considered variants of normal development, The ossification changes are usually spontaneously corrected after weaning
There have been isolated reports of birth defects among babies born to women exposed to topical tertinoin during pregnancy , to date, there have been no adequate and well-controlled prospective studies performed in pregnant women and the teratogenic blood level of tretinoin is not known, However, a well-conducted retrospective cohort study of babies born to women exposed to topical tretinoin during the first trimester of pregnancy found no excess birth defects among these babies when compared with babies born to women in the same cohort who were not similarly exposed, topical tertinoin should be used during pregnancy only if the potential benefit justifies the potential risk to the fetus, it is not known wether tretinoin is excreted in the human milk, Since mny drugs are excreted in human milk, caution should be exrecised, When Retin-A is administered to a nursing mother
Undesirable effects
Some degree of local irritation is expected, The most commonly reported undesirable side effects are dry skin, burning, stinging, warmth, erythema, pruritus, rash, peeling and temporarily hypo & hyper-pigmentation
Rarely reported undesirable effects are blistering and crusting of the skin, eye irritation & edema, True contact allergy to topical tretinoin is rarely encountered
Some degree of local irritation is expected, The most commonly reported undesirable side effects are dry skin, burning, stinging, warmth, erythema, pruritus, rash, peeling and temporarily hypo & hyper-pigmentation
Rarely reported undesirable effects are blistering and crusting of the skin, eye irritation & edema, True contact allergy to topical tretinoin is rarely encountered
Interactions
Concomitant topical medication, medicated or abrasive soaps and cleansers, soaps and comsmetics that have a strong drying effect, and products with high concentration of alcohol, astringents, spices or lime should be used with caution because of possible interaction with tertinoin, Particular caution should be exercised in using preparations containing sulphur, resorcinol, or salicylic acid with Retin-A, It is also advisable to "rest" a patient’s skin until the effects of such preparations subside before use of Retin-A is begun
Concomitant topical medication, medicated or abrasive soaps and cleansers, soaps and comsmetics that have a strong drying effect, and products with high concentration of alcohol, astringents, spices or lime should be used with caution because of possible interaction with tertinoin, Particular caution should be exercised in using preparations containing sulphur, resorcinol, or salicylic acid with Retin-A, It is also advisable to "rest" a patient’s skin until the effects of such preparations subside before use of Retin-A is begun
Overdosage
Topical application of Retin-A is characterized by little systemic absorption, hence overdosage is unlikely
Retin-A is intended for topical use only, In the event of accidental ingestion, if the ingestion is recent, the stomach should be emptied immediately by gastric lavage or by induction of emesis, All other treatment should be appropriately supportive, Oral ingestion of Retin-A may lead to the same adverse events as those associated with excessive intake of vitamin A
Topical application of Retin-A is characterized by little systemic absorption, hence overdosage is unlikely
Retin-A is intended for topical use only, In the event of accidental ingestion, if the ingestion is recent, the stomach should be emptied immediately by gastric lavage or by induction of emesis, All other treatment should be appropriately supportive, Oral ingestion of Retin-A may lead to the same adverse events as those associated with excessive intake of vitamin A
Storage Conditions
Cream: store at or below 25 degree C
Gel: store at or below 25 degree C
Solution: store at or below 25 degree C, protect from light
Cream: store at or below 25 degree C
Gel: store at or below 25 degree C
Solution: store at or below 25 degree C, protect from light
Supplied
0.01%: 15g Gel
0.025%: 15g, 30g Gel - 20g\30g Cream
0.05%: 20g\30g Cream
0.1%: 20g Cream \ 15ml solution
Dispensed in pharmacies on physician’s prescription
0.01%: 15g Gel
0.025%: 15g, 30g Gel - 20g\30g Cream
0.05%: 20g\30g Cream
0.1%: 20g Cream \ 15ml solution
Dispensed in pharmacies on physician’s prescription
ليست هناك تعليقات:
إرسال تعليق